This post may contain affiliate links. Please see our disclosure policy.
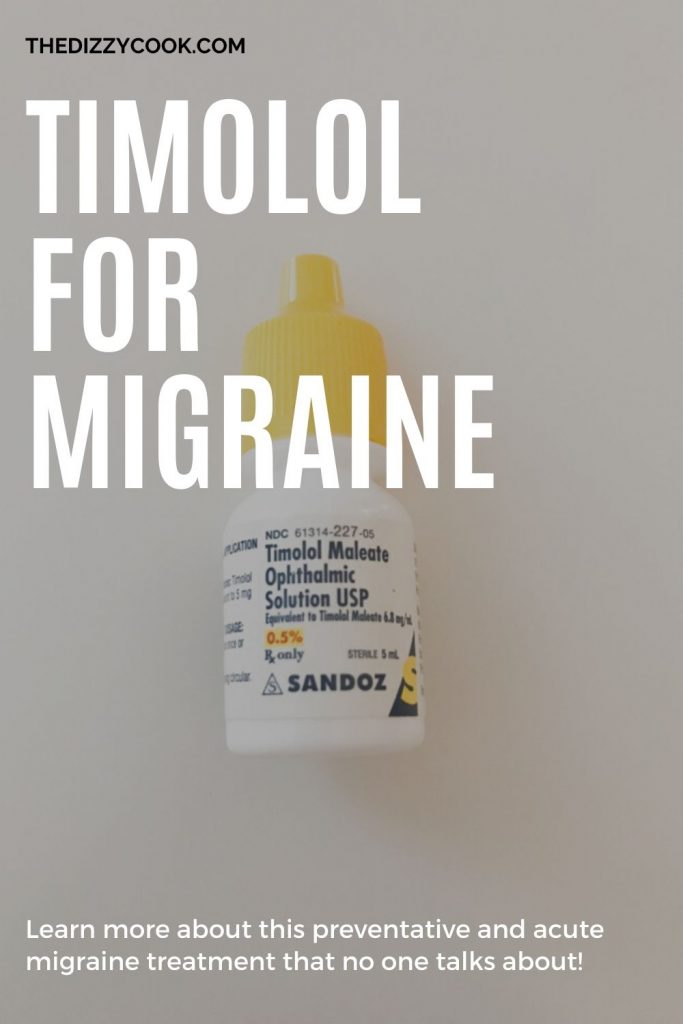
I wanted to share my patient experience with timolol drops for migraine in case it may help others. I have been using timolol malate ophthalmic solution for the past three years as both a vestibular migraine preventive and, most recently, as an acute treatment. This post was originally published July 22, 2019 and recently updated on December 30, 2020 with new research via Dr. John Hagan.

When my neurologist first prescribed this medication, like any curious patient I took to the internet to search through everything I could about it. I checked all my migraine support groups, yet I could find nothing on timolol drops for migraines. There was some info on the pill form, but not much on the drops. It seemed like I was the only person in the world on this particular medication. Beta blockers in pill form, like propranolol, have been used for years to treat migraine disorders, yet this was a method that seemed to be rarely used.
At my following appointment with Dr. Beh, I asked him why he recommended it to me. He mentioned that there’s a tendency for beta blockers to have greater side effects when in pill form, but as an eye drop it can be absorbed quickly into the blood stream, making a very small amount of medication highly effective. Used in this form, I could have faster relief but with lowered risk of side effects.
Research on Timolol Malate
The first study on the use of beta blocker eye drop treatment of headaches was in 1980, however, not much had been followed up with it until 2014. In studies, timolol in pill form has been found to be just as effective as propranolol in migraine prevention at 20-30mg a day. Yet with the oral dosage of beta blockers being the most popular prescription, it absorbs too slowly to be considered an acute treatment. Timolol received FDA approval in 1978 for the treatment of glaucoma, and when used as eye drops, patients would report the added benefit of a reduction in migraine attacks.
Ophthalmologists Hagen and Migliazzo put these observations together and published a study in 2014 in The Journal of the Missouri State Medical Association. Five out of their seven patients reported complete pain relief, while the other two reported a significant reduction in pain relief when used in their acute migraine attacks. The idea is that beta blocker eye drops reach therapeutic levels within minutes of application without causing unwanted side effects.
- In 2018, a study of patients who met the International Headache Society’s requirements for migraine received timolol maleate eye drops in 0.5% dosage, a single drop in each eye, at the onset of symptoms and once again 30 minutes after. The study took place over a 4 month period, where ten patients scaled their pain from 0 to 3, and rated the effectiveness of the drops when used for their attacks. Timolol was rated at a 2.4 in effectiveness when the placebo was rated at 1.4.
- Four of the patients rated this treatment as highly effective and only one had an adverse reaction to the treatment. Of all the migraine attacks reported, 37 out of 55 had no symptoms to mild symptoms when the timolol treatment was used early.
- In 2019, Dr. Carl Migliazzo and John Hagan III called for more research into this promising medication and shared a story from Carolyn Csongradi, who had tried a multitude of migraine medications with terrible side effects from propranolol to nortriptyline. With her mild persistent asthma, she could not take Imitrex-type drugs or other oral beta blockers. Although typically not recommended for asthma, her neurologist agreed to let her try 2 drops of 0.25% a day in each eye. It has proven to be a successful abortive medication for her without side effects or a negative impact on her asthma.
- In 2020, Dr. Bradley J. Katz published an article on JAMA Ophthalmology called “Pulled a Drop of Timolol Into Each Eye and Call Me in the Morning” recommending Timolol as “inexpensive” and a “very good adverse event profile and safety profile”. It also called to attention the observations of the authors that there may be even larger benefits as a nasal spray because of the rapid absorption, similar to Sumatriptan.
- In May-June 2020, Dr. John C. Hagan III along with Eric Everett, RPh and Tyler Chamberlain discussed using Timolol sublingually as well as a nasal spray. They recommend the nasal spray for those who have trouble properly doing the eye drops, perhaps cause of the stinging sensation. Their research shows nasal administration to be the fastest absorbed and most effective. However, currently you can only get this prescribed through them (available through O’Brien Pharmacy)
Side Effects
The current medications used in acute treatments, like NSAID’s and triptans, come with a risk of rebound attacks when used too often. Since beta blockers are already used as a daily migraine preventative treatment, it’s likely they wouldn’t carry that same risk.
Side effects of traditional beta blockers can include lower blood pressure or an adverse effect on asthma. However, the dosages in pill forms are much higher than what can be taken in the eye drop form, meaning there would be a lowered risk of these potential side effects. Also, if taken as an abortive and not a preventative medication, some with low blood pressure find they can tolerate it well.
As you can see above, patients with asthma have been able to use them without adverse reactions. My vestibular migraine friend who is also a patient of Dr. Beh’s, Kayla McCain, manages to use them without and adverse effect on her asthma (although our physician, and myself, had to really twist her arm on trying it!).
Since these drops are used often for glaucoma, it should come with little to no risk to the eyes, however a meeting with an ophthalmologist is always essential. In the beginning, I found the drops stung for a few seconds when first applied, yet it quickly went away. If this is an issue for you, you could try Dr. Hagan’s suggestion to use them sublingually or contact their pharmacy to check on the nasal spray. The nasal spray is $30 plus postage.
Timolol for Vestibular Migraine
I was prescribed the 0.5% solution with instructions to take it 2x a day, at night and in the morning as a preventative medication. Then I could use it as needed, as an acute medication, for bad attacks. It did take a while for me to notice a reduction in symptoms, a couple of months at least. However, I was not the kind of patient who expected results overnight. I stayed the course and kept doing what I was supposed to. I think what helped me the most was combining these drops with other preventative measures, like diet and supplements.
Now that my vestibular migraine is fairly well controlled, I use the timolol eye drops as an abortive or rescue medication. Just a drop in each eye when I feel my dizziness kick up seems to help ease my head a bit and lessen an attack. I find this is also true for my other friends with head pain associated with their migraine.
Since I started taking it several years ago, I spread the word about how much it was helping me and now several migraine friends are finding success as well.
A Note on Pregnancy
My OB has approved these as an acute medication and a preventative for post pregnancy. Beta blockers are typically one of the approved meds, should women with migraine need the option. You can read more about my experience using them while trying to conceive. This is a big reason why I made them apart of my original treatment plan.

Talking to Your Neurologist about Timolol Drops
So why did it feel like I was the only person in the world on it? First of all there wasn’t a ton of research on it at the time, even though the research out there is positive, so a lot of the successful feedback came from Dr. Beh’s own patients like myself.
The other reason? Money. Pharmaceutical companies don’t really want to invest in a drug that they cannot market. There’s more money involved with all the new anti-CGRP treatments and Botox, which means more research. For a generic eye drop, it’s not going to get a lot of attention or money invested into it. (If you check out this study, don’t miss all the ads for anti-CGRP or Botox that surround it and you’ll see what I mean.) Dr. Hagan recently reached out to me in December 2020 to mention he has been trying to get Big Pharma to develop this medication over the past 6 years.
If you’re curious to try this treatment, I recommend printing out all the studies and approaching your neurologist about it. The feedback I typically hear is that they have either never heard of this, or the trials weren’t large enough to prove anything significant. While that might be true, there are lots of treatments when it comes to migraine, especially vestibular migraine, that aren’t backed by massive studies. I feel that it’s these small, yet very positive, studies that can make a huge difference in some of our lives. It certainly did for me!
A big thank you to Dr Hagan for providing these linked updated articles and materials, as well as pushing for this medication for our community.
Other Articles on Timolol and Migraine
For more posts on vestibular migraine and other articles using Timolol for migraine management, see these articles:
Vestibular Migraine Symptom Guide
Acute Treatments for Vestibular Migraine
5 Ways to Relieve a Migrainous Vertigo Attack
TTC and Pregnancy with Migraine
My Vestibular Treatment Plan
Referenced materials:
1. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6312165/
2. https://jamanetwork.com/journals/jamaneurology/article-abstract/2680666
3. https://headaches.org/2016/07/01/use-beta-blocker-ophthalmic-solution-treatment-migraine/
4. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/neurology/headache-syndromes/
5. https://www.ncbi.nlm.nih.gov/pubmed/2879629
6. https://www.neurologylive.com/clinical-focus/timolol-migraine-shows-efficacy-abortive-therapy
7. https://www.msma.org/uploads/6/2/5/3/62530417/beta_blocker_for_migraines_julyaug2014_momed.pdf








Do you. Know. Of a doctor in Jackson New Jersey area
Hey! Here are my doctor recommendations. There are some online if there aren’t any near you.
Alicia: Hello again. This is Dr. John C Hagan III. We have just published the first world report of using timolol eye drops in a nasal spray for the successful treatment of 63% of very difficult migraine patients referred to a headache clinic in Kansas City. All had failed primary and secondary migraine abort medication failure. My collaborator is Steve Kosa MD a neurolgist that runs the clinic. Timolol 0.5% nasal spray is available from O’Brien Pharmacy in Kansas City, Bayview Pharmacy in Rhode Island and Health Diminisions Pharmacy in Michigan. Any competent compounding pharmacy can prepare the nasal spray using directions we published in Int J of Phar Compounding LINK https://digitaleditions.walsworth.com/publication/?i=815984&p=34&view=issueViewer
Alecia hello this is John C Hagan III MD the developer of timolol eye drops for acute migraine. I would like to send you some updated information and new researcch. The timolol is now available as an inexpensive nasal spary. My email address is drjhagan3@gmail.com
This is the particular bottle that my Timolol is packaged in and.the last 3 bottles I’ve gotten the fluid wants to pour out of it. The hole at the top is too big. I don’t know if this is the place to address this at but here it is. This is a concern for several obvious reasons.
Hey Shelley, I would bring this to the attention of your pharmacy!
Great article! Dr. Beh just prescribed these so I can try them.
Fingers crossed they help as part of my treatment pie.
Always appreciate your willingness to share your experiences.
Hi!
Can these drops help for cluster type headaches. One eye one eyebrow involvement. Great articles!! Thank you for sharing!!
Laurie
Hey Laurie, I’m really not sure, that might be a better question for your dr. However, I would also recommend looking into gammacore. I know they specifically have a program for cluster headaches. I also have a discount code “dizzycook” for 15% off if you decide to try it.