This post may contain affiliate links. Please see our disclosure policy.
What is PPPD, or Persistent Postural-Perceptual Dizziness, and how do you treat it? How is it different from Vestibular Migraine or other vestibular disorders?
If you get daily dizziness that seems to never change, this could be an issue you face along with Vestibular Migraine. But how do doctors distinguish between the two when you have both?
Triple PD or “three PD” is a very new diagnosis that has only been recently recognized by the World Health Organization in 2017. Therefore, like most other vestibular disorders, patients may have to do some research to find a doctor that is familiar with this diagnosis. VEDA is a resource that can help.
Table of Contents
Symptoms of PPPD
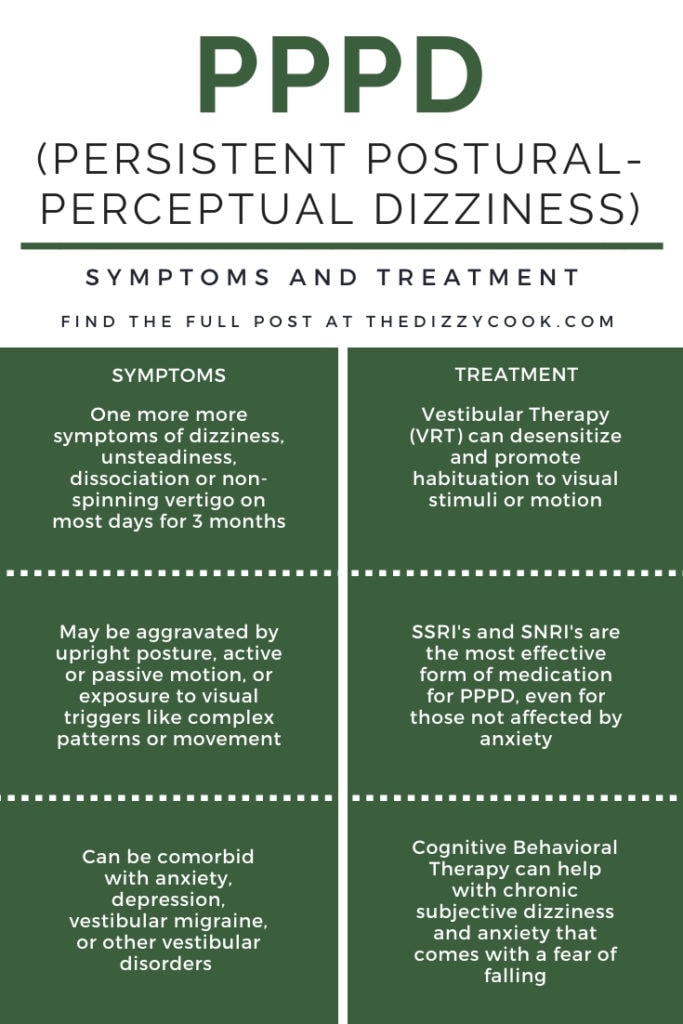
As many vestibular disorders can mimic each other, you’ll often see people question a diagnosis. PPPD, Persistent Postural-Perceptual Dizziness, is typically accompanied by symptoms of dizziness, unsteadiness, and non-spinning vertigo.
The criteria for diagnosis is that symptoms are present on most days for three months or more and can be aggravated by upright posture and increased visual stimulation through movement or complex patterns. Unlike Vestibular Migraine, which can have episodes of vertigo or intense symptoms, PPPD is a steady level of dizziness. But most often, patients have both.
Sometimes symptoms can be decreased through distraction or randomly disappear. They do not have to be continuous throughout the entire day, but can also appear for hours at a time. These episodes can originate from the brain (neurological) or be vestibular related (the inner ear). They can also come with an initial reaction of high anxiety and a fear of being suddenly imbalanced.
Some things that may increase PPPD symptoms are :
- Normal movements like standing or walking.
- Looking at traffic or any areas with movement
- Walking through a crowded grocery store
- Using a computer or phone and scrolling
- Sitting in a busy restaurant
What Causes Triple PD
This disorder can either start very obviously with an acute event, or develop slowly with a chronic event, however, the acute event is much more common. With an acute event, the symptoms might be episodic at first before becoming a pattern. There must always be a cause for PPPD to occur as it is not a stand alone diagnosis.
These acute events could be:
- Another peripheral vestibular disorder like BPPV
- A panic attack
- A neurological disorder like Vestibular Migraine
- Concussion or whiplash (perhaps from a car accident)
Chronic events could be:
- Another vestibular disorder that can be chronic like Meniere’s Disease or Vestibular Migraine
- A disease of the autonomic nervous system (or Dysautonomia)
For these events, symptoms may come on slowly and then become more persistent. See the Bárány Society diagnostic criteria for more details.
It appears that in a quarter of the cases, the event is caused by a peripheral or central vestibular disorder like BPPV or vestibular neuritis and in 20% of cases, it’s caused by vestibular migraine. (Staab JP, Eckhardt-Henn A, Horii A 2016)
How Persistent Postural-Perceptual Dizziness is Diagnosed
Bárány Society diagnostic criteria must be fulfilled so this will involve your doctor closely examining your history. Was there any major events this could be triggered by? What are the symptoms you’re experiencing and have you had them for 3 months?
Another difficult aspect is many of these symptoms crossover with vestibular migraine. You may feel a sense of motion without spinning (vertigo), have lightheadedness or a feeling like you’re swaying or “on a boat”. There’s also dissociation where you could feel like you’re floating or where you feel “out of it”. Dr. Edward Cho mentions that in his practice dissociative symptoms are actually a huge clue that PPPD is present.
Your doctor might also ask you what increases and decreases your symptoms. Do you feel worse walking in hallways with patterned carpets? Or do you search for one spot to keep yourself steady? A patient with Persistent Postural-Perceptual Dizziness may be highly dependent on visual cues.
Other vestibular tests may be performed to rule out other conditions, or help your doctor decide what other disorders coexist with PPPD. You can most definitely have BPPV and PPPD or Vestibular Migraine and PPPD. Unfortunately for some, Persistent Postural-Perceptual Dizziness is diagnosed as a catch all term when doctors have no idea how to decipher a patient’s dizziness.
The Anxiety Connection
When a patient does not use an appropriate cognitive behavioral response by thinking this is just a moment and they are safe, it adds “a secondary psychological and functional morbidity, such as fear of falling, anxiety, or depressive disorders, and functional gait abnormalities” according to research from Popkirov, Staab, and Stone. The term “gait abnormalities” basically means you walk oddly. Perhaps this is because you feel as though the ground is moving or like you’re walking on sponges. This is also a symptom of other vestibular disorders, like vestibular migraine.
While PPPD does not actually cause anxiety, anxiety and PPPD can exist closely together as a comorbidity. In fact a patient who is prone to anxiety and depression is 60% more likely to develop PPPD.
Because of the anxiety factor, many patients may need counseling as they become fearful to do certain activities and this can lead to bad habits. Not exercising, moving, or cooking(!) can be harmful in the long term.
How is PPPD Treated?
Obviously this will depend on your specific case and whether or not you’re treating a comorbidity, but the most common practices are:
- Vestibular Therapy – this is started very slowly and slightly increased with time. The idea is to reduce visual triggers and abnormal responses through movements and tasks. This promotes habituation, which allows you to be less sensitive to visual stimuli.
- SSRI’s and SNRI’s -selective serotonin reuptake inhibitors and selective serotonin norepinephrine reuptake inhibitors (typing that just did a NUMBER on my spell check…red lines all over!) seem to be the most promising medications for PPPD. You must understand that these aren’t just treating the anxiety, but actually treating PPPD. You do not have to have anxiety to benefit from this medication. However, they can also improve the comorbidity of anxiety and depression.
- In clinical practice, SSRI’s are usually started first and then SNRI’s are introduced if not effective or not tolerated well.
- SSRI’s and SNRI’s can be expected to have a response within 8-12 weeks. If these are found to be beneficial for the patient, treatment is typically continued for at least one year.
- The most popular is Effexor ER/Venlafaxine, which begins at 37.5mg for dosage. But microdosing can help mitigate side effects. This would involve a schedule of breaking open the capsule and taking a certain amount of the beads. This must be done under the guidance of a neurotologist, neurologist or ENT.
- CBT – Cognitive Behavioral Therapy – More recent studies have showed CBT can lead to up to a 75% improvement in some patients with chronic subjective dizziness, which seemed to continue at 1 and 6 months of treatment. (E J Mahoney A, Edelman S, D Cremer P. 2013). CBT can also help with the anxiety comorbidity and help patients who fear falling or the perceived risks associated with dizziness.
- gammaCore or Truvaga – Any non-invasive vagus nerve stimulation could help if anxiety or migraine is a component.
Some of the effective treatments for vestibular migraine are also effective for PPPD.
Early Diagnosis is Beneficial
Although it can be tough to find a physician who is skilled at distinguishing vestibular disorders and diagnosing PPPD, it appears to be incredibly important to the overall long term success of treatment.
It appears that starting treatment early can lead to a greater benefit long term for the patients and yield a higher success rate. Years of dealing with chronic dizziness can indicate a more severe disability and an acceptance of the illness as everyday life. (Dieterich M, Staab JP, Brandt T. 2016) This is why it’s important to be your own advocate when it comes to your appointments and continue to ask questions. It may even be necessary to travel to find an appropriate doctor, but most often the effort will be rewarded.
More PPPD Information
For more detailed information, see my youtube video on PPPD with Dr. Edward Cho.
References:
- Staab JP, Eckhardt-Henn A, Horii A, et al. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): consensus document of the committee for the classification of vestibular disorders of the bárány society. J Ves Res 2016
- E J Mahoney A, Edelman S, D Cremer P. Cognitive behavior therapy for chronic subjective dizziness: longer-term gains and predictors of disability. Am J Otolaryngology 2013;34:115–20.
- Dieterich M, Staab JP, Brandt T. Functional (psychogenic) dizziness. Handbook Clinical Neurology 2016;139:447–68.
- Thank you to Dr. Edward Cho from House Clinic for providing some of these materials and clinical experience.








Hey I thought I’d leave this for people I’ve had this illness for over 5 years and I know it’s brutal you often feel like you’re losing your mind or that it’s in your head and it’s not and you’re not alone there is not a cure for this problem really but the treatments can help a lot I’m currently on citalopram and it’s made it to where I can have a life again it’s not perfect but don’t lose hope it takes strength to push through this illness working out is also a massive help you may feel awful doing it but you need to also DONT feel to bad about gaining weight with PPPD food often helps with nausea so it makes since you would gain pounds that doesn’t make you a slob your battling an illness where often the only time you feel ok is when you’re eating drink lots of water and take yourself away from stressful situations learn to keep calm your anxiety cause anxiety makes it hundred times worse Either way good luck and keep pushing through
Hello i got PPPD for almost 3 moths now im on SSRI. Is it posaible to fully recover from that its soo bad. I maybe feel a little bit better. What exercise should i do and anything else to help me recover
Hey – it is possible to recover! It can sometimes just take a little while. There are no specific exercises, but movement in general can be helpful. Usually a vestibular therapist can work with you if certain positions are causing an increase in symptoms. But more than that, I’d look into a psychological therapist to help with mindset and different therapy techniques that may help.
Hi, can share about your PPPD symptoms and what you encountered or experience daily? I am not sure about if i am having PPPD and doctor are unsure and keep asking to go for MRI. How your doctor examine your condition and confirm you are having PPPD?
Finding this has been very helpful! I’ve ordered both of your cookbooks which should arrive in the next week or so. I’m a bit stuck and wonder if you might have encountered a bit of a unicorn diet… I’m trying to help a family member who has celiac disease and is a vegetarian and now needs to include low-glutamate due to a recent diagnosis of vestibular migraine and 3PD. The doctor gave a list of foods to avoid and recommended your cookbooks as a starting place. (We live outside of North America with limited access to resources.) My major concern is trying to find more variety of proteins beyond endless cans of beans.
Hi Alicia,
I’ve followed your page for some time. Do you think you had PPPD somewhere in your journey? I had vestibular neuritis and likely PPPD. I’m now finding when I decompensate the PPPD returns. I’m working with my friend physical therapists again. Just curious if you think you recovered from PPPD over time with exercises, life and therapy?
Hey! Yes, we do think that I had PPPD with VM, it just wasnt really diagnosed back when I was diagnosed with VM. I did recover from PPPD with vestibular migraine treatment. Eventually once my attacks calmed, the background dizziness slowly went away.
Hi. My son was recently diagnosed with PPPD. He currently resides in Charlotte, NC and we are having difficulty finding a CBT who has experience with this disorder. Do you know of anyone in his area?
Thanks.
Hey Alvin, I don’t unfortunately, I imagine there are very few people. I would recommend reaching out to Kristi (her info is in the post) or Rooted Behavioral Education. Both are vestibular disorder patients who work in counseling! 🙂
I just wanted to say thank you so much to Alicia for posting this, and for everyone above sharing their experiences. I’d never heard of this before but reading through it sounds exactly what I have been suffering with for several years now. The feeling of understanding and possibility that it could be treated is incredible, I could cry. Am going to talk to my doctor about this and hopefully we’ll make some progress. Thank you.
I hope you get the answers you need!
i am from mexico am 31 years old now. mexico as been a third world country is hard to find information about this kind of migrane The VM i have a cuestion does your Dc. can treatme by line
sorry for my bad inglish hope a good day for you and your fsmily